
At the end of March, much of the national focus around COVID-19 was on case numbers and rising mortality in London as well as bed capacity in the NHS.
This was logical as London was the initial epicentre for the disease and the health service the obvious frontline. But, given the uncertainty about actual case numbers, the likelihood of it spreading across the nation, and underlying health vulnerabilities in different places, there was a risk of blindly following cases rather than taking a forward look at the places most at risk of high mortality should the surge reach them.
Over the course of April, the CPP’s COVID-19 Health Index has sought to provide this forward look by striking a balance between accounting for the systemic vulnerability of local areas and the present reality of rising COVID cases. This meant putting much greater emphasis on the existing health of a local area’s population, the ability of the healthcare system to treat common conditions such as respiratory illness, the proportion of older people living in an area and crucially, the strength of the adult social care system. The tragedy of repeatedly kicking this policy can down the road is now all too apparent.
By focusing on underlying vulnerability, the map of the riskiest places moved away from London and towards the Midlands and North of England. In early April, the West Midlands became the new battleground against the disease with five of its local areas ranked in the top 15 riskiest places. It was around this time that Government fast tracked the construction of the Birmingham Nightingale hospital.
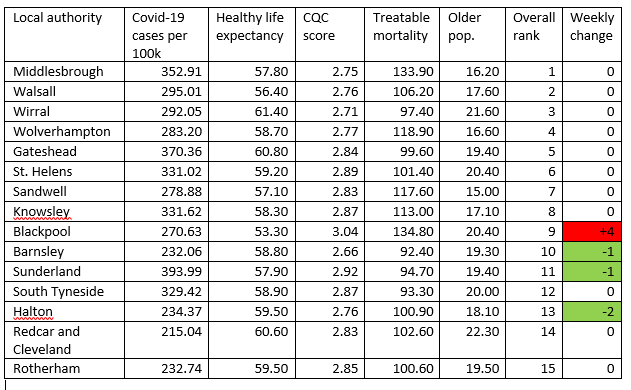
Over the month, the focus of our index moved to the North East which has seen large rises in cases combined with a high level of underlying vulnerability. Middlesbrough has come out on top of the index as the riskiest place for the last three weeks.
It is one of the most deprived local authorities in the country, has significant underlying health issues and (until recently) a rising case load. This prompted the mayor to keep parks closed in the area and sparked a fierce debate about national versus local intervention in response to the health crisis. In this sense, there are no easy decisions with tough trade-offs between what is most likely to save lives from COVID-19 now, versus serious considerations about mental and physical health and the likely behavioural responses to continued public health restrictions.
One surprise over the month is that despite the lockdown being a nationwide policy, different local areas have seen significantly different growth rates in cases. We think part of the answer to this lies in the number of cases at the start of the month – those areas with fewer initial cases were more likely to see a larger increase. But the answer is also related to the structure of the workforce – those areas with jobs more easily done from home were less likely to see rapidly rising cases. Homeworking – or lack of it – may also be linked to the rate of spread in the disease itself.
What this crisis has underlined is the holes in local institutional resilience. Public health has been long ignored. Alongside this public health deficit, there is a national catastrophe playing out before our eyes in adult social care. It is thought that around half of all deaths related to COVID-19 may be in the community and care homes – a sector ill-prepared for such a crisis, having been under-resourced and under-valued for so long.
The Nightingale hospitals were a strong and bold signal of the Government’s seriousness about the NHS’s ability to cope. By contrast, adult social care workers get to wear a badge.
Sometimes a summary statistic can say it all – 60% of all domiciliary care workers are on a zero hours contract. This is truly shocking. As we emerge from this crisis, embracing critical local institutions which serve to reduce pressure on the health service and support long-term social and economic wellbeing must be prioritised to strengthen community resilience. There simply is no alternative.
Ben Franklin is head of research at the Centre for Progessive Policy